GLP-1 Weight Regain: How to Keep the Weight Off After Stopping Ozempic, Mounjaro, or Retatrutide
The Bottom Line
Stopping a GLP-1 like semaglutide, tirzepatide, or retatrutide without a plan is one of the most common ways people undo months of progress. Studies show that 60-67% of weight lost comes back within the first year after discontinuation. The good news: weight regain isn't inevitable. It requires a real exit strategy that includes tapering (not cold turkey), locking in lifestyle changes while still on the drug, and tracking the right signals during the transition. This guide covers why regain happens, how to prevent it, and when it makes sense to restart. Use the Regimen app to track your weight trends, body composition, and protocol changes so you can catch regain early and adjust before it spirals.
In this guide:
- The Weight Regain Problem: What the Research Actually Shows
- Why Weight Comes Back After Stopping GLP-1s
- Tapering vs Cold Turkey: Why How You Stop Matters
- The Maintenance Dose Approach
- Lifestyle Anchors That Lock In Your Results
- Tracking Your Maintenance Phase
- When to Restart vs Adjust
- The Psychological Side of Stopping
- FAQs
The Weight Regain Problem: What the Research Actually Shows
If you've been on Ozempic, Mounjaro, Zepbound, or compounded retatrutide for a while and you're thinking about stopping, you've probably already seen the scary headlines. And unfortunately, the data backs them up.
The STEP 1 trial extension found that participants who stopped semaglutide regained about two-thirds of the weight they had lost within one year of discontinuation. The SURMOUNT-1 extension data for tirzepatide showed a similar pattern. People lost an average of 20.9% of body weight on the drug, then regained about 14% in the year after stopping.
Those numbers are real. But they're also averages, and they include people who stopped with zero plan. No taper. No lifestyle changes locked in. No monitoring. Just stopped taking the drug and went back to life as usual.
The people who kept the most weight off had a few things in common: they had established exercise habits before stopping, they were eating adequate protein, and they had a system for catching small regain early instead of waiting until it became a big problem.
Why Weight Comes Back After Stopping GLP-1s
To prevent regain, you need to understand why it happens. There are three main drivers, and they all hit at once when you stop.
Appetite Hormone Rebound
GLP-1 medications suppress ghrelin (your hunger hormone) and enhance satiety signaling. When you stop, those appetite signals come roaring back. Most people describe it as "the food noise returning," and it often feels more intense than it did before starting treatment.
Your brain was receiving a constant signal that you were satisfied. Remove that signal, and there's a rebound effect. Hunger doesn't just return to baseline. For many people, it temporarily overshoots. This is why the first 8-12 weeks after stopping are the highest risk period.
Metabolic Adaptation
Your body lost significant weight. That means your resting metabolic rate dropped. A person who now weighs 180 lbs after losing 50 lbs burns fewer calories than someone who has always weighed 180 lbs. Your body adapted to the lower calorie intake during treatment, and that adaptation doesn't reverse just because you stopped the medication.
This metabolic penalty can persist for months or even years. It means the margin for error is smaller than you'd expect.
GLP-1 Receptor Downregulation
Your body got used to having elevated GLP-1 receptor activity. When you remove the exogenous source, your natural GLP-1 production hasn't increased to compensate. It takes time for your body's own incretin system to readjust. During that gap, your blood sugar regulation and satiety signaling operate below where they were before you ever started the drug.
Tapering vs Cold Turkey: Why How You Stop Matters
Most people who regain weight rapidly made the same mistake: they stopped their GLP-1 abruptly. Maybe their prescription ran out, maybe insurance stopped covering it, maybe they hit their goal weight and figured they were done.
Cold turkey discontinuation hits your system hard. You go from full receptor activation to nothing overnight. That's when the rebound hunger hits hardest.
A gradual taper gives your body time to readjust.
A Practical Taper Protocol
There's no FDA-approved tapering schedule for GLP-1s (the clinical trials studied on/off, not tapered discontinuation), but the approach most clinicians use looks something like this:
For semaglutide (Ozempic/Wegovy):
- If on 2.4mg, step down to 1.7mg for 4 weeks
- Then to 1.0mg for 4 weeks
- Then to 0.5mg for 4 weeks
- Then to 0.25mg for 4 weeks before stopping
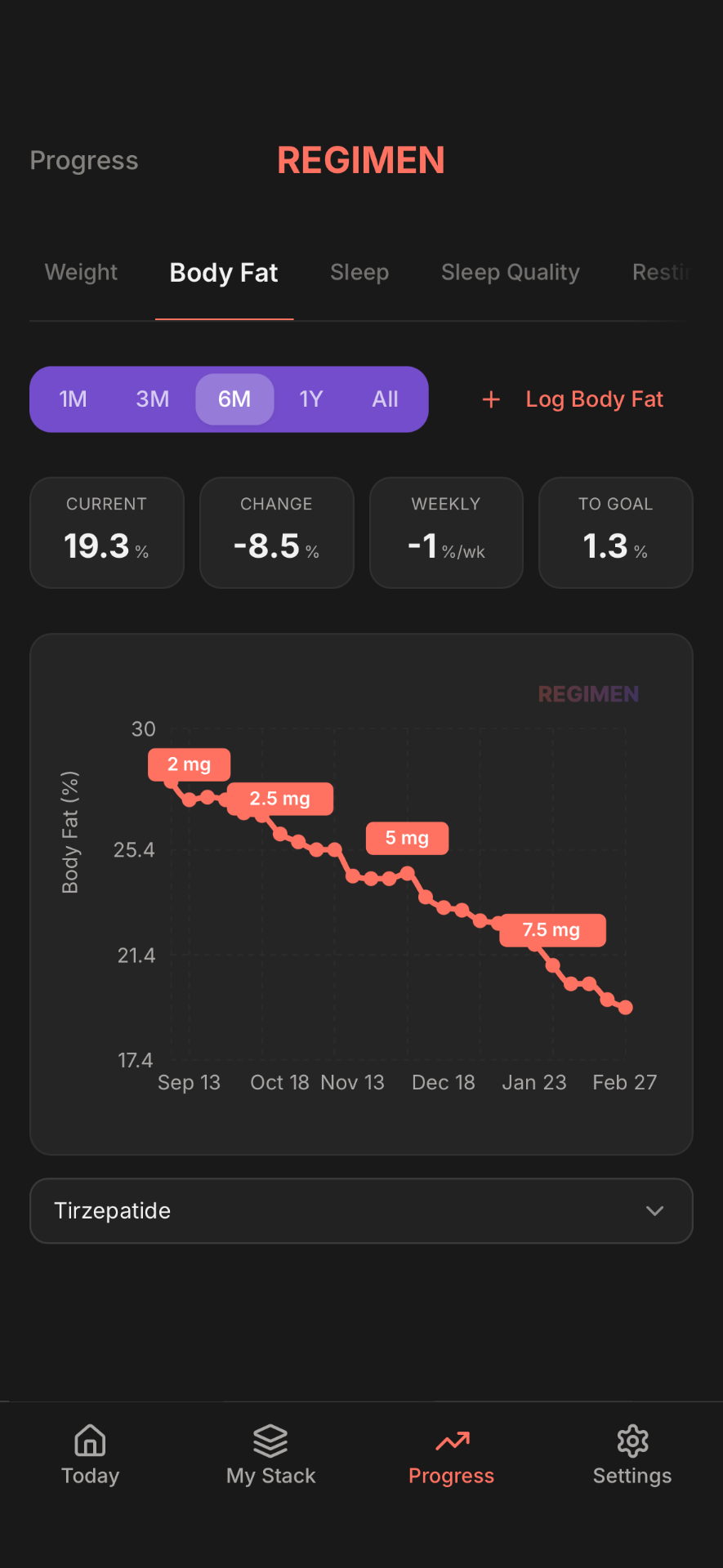
For tirzepatide (Mounjaro/Zepbound):
- Step down one dose level every 4 weeks
- From 15mg to 10mg to 7.5mg to 5mg to 2.5mg
For retatrutide (compounded):
- If on 12mg, step down to 8mg for 4 weeks
- Then to 4mg for 4 weeks
- Then to 2mg for 4 weeks before stopping
Retatrutide has a triple agonist mechanism (GLP-1/GIP/glucagon), so the metabolic adjustment during tapering may feel different than semaglutide or tirzepatide. The glucagon component means your body has additional metabolic pathways to recalibrate. Tapering slowly is even more important to avoid a sharp rebound.
Each step gives your body about a month to adjust before the next reduction. You'll likely notice some increase in appetite at each step, but it's manageable compared to going from full dose to nothing.
The Maintenance Dose Approach
Here's something the conversation around GLP-1s is starting to shift toward: maybe stopping completely isn't the goal for everyone.
Think of it like blood pressure medication. Nobody says "great, my blood pressure is normal now, time to stop the medication." Obesity is increasingly recognized as a chronic condition, and for many people, a long-term maintenance dose makes more sense than full discontinuation.
A maintenance dose means staying on the lowest effective dose rather than stopping entirely. For semaglutide, that might be 0.25mg or 0.5mg per week. For tirzepatide, it could be 2.5mg or 5mg. For retatrutide, early community experience suggests 1-2mg weekly as a maintenance range, though this will become clearer as more data emerges.
The advantages are real:
- Continued appetite regulation (even low doses provide meaningful satiety support)
- Prevention of metabolic rebound
- Much better weight maintenance outcomes compared to full discontinuation
- Lower cost than therapeutic doses
The downside is that you're still on the medication indefinitely. For some people, that's a perfectly reasonable trade-off. For others, particularly those concerned about long-term unknowns, full discontinuation with a solid lifestyle plan is preferred.
Lifestyle Anchors That Lock In Your Results
Whether you're tapering off completely or stepping down to a maintenance dose, these habits need to be established before you reduce your medication. Not after. Before.
Protein has the highest thermic effect of any macronutrient (your body burns 20-30% of protein calories just digesting it), provides the strongest satiety signal per calorie, preserves lean mass, and blunts blood sugar spikes. Target: 1.2-1.6g per kg of body weight, minimum. Front-load it: aim for 30-40g at your first meal.
Lifting weights preserves and builds lean mass. More lean mass means a higher resting metabolic rate, directly counteracting the metabolic penalty from weight loss. Minimum effective dose: 2-3 sessions per week focusing on compound movements (squats, deadlifts, presses, rows).
Poor sleep increases ghrelin (hunger hormone) by up to 28% and decreases leptin (satiety hormone) by 18%. One bad night of sleep can increase next-day calorie intake by 300-400 calories. When you're no longer on a GLP-1 suppressing your appetite, those sleep-driven hunger spikes hit much harder. Target 7-9 hours per night.
Non-exercise activity thermogenesis (NEAT) accounts for 200-500 calories per day. After weight loss, NEAT tends to decrease naturally. Consciously maintaining a daily step target of 8,000-10,000 steps helps offset this. More on protecting lean mass.
Tracking your GLP-1 taper? Regimen makes it easy
- Log dose changes, weight trends, and body measurements
- Track appetite scores alongside your protocol
- See exactly how your body responds to each adjustment
Tracking Your Maintenance Phase
The people who successfully keep weight off after stopping GLP-1s all share one habit: they monitor. Not obsessively, but consistently.
Weight trends, not daily weight
Your weight fluctuates 2-5 lbs day to day. A single weigh-in tells you almost nothing. A 4-week trend tells you everything. Weigh yourself daily at the same time and look at the weekly average. If your 4-week rolling average is trending up, that's the signal to act.
Body measurements
Waist circumference is particularly useful because it tracks visceral fat changes that the scale misses. Measure at the navel, same time of day, once per week.
Appetite signals
Rate your hunger on a 1-10 scale each day. Rising appetite levels over several weeks can predict weight regain before it shows up on the scale. This is your earliest warning system.
Protein intake
Track this daily for at least the first 3 months after stopping. Most people overestimate their protein intake by 20-30%.
When to Restart vs Adjust
You've been off your GLP-1 for a few months and the scale is creeping up. How do you decide between lifestyle adjustments and restarting medication?
Try Adjustments First If:
- You've regained less than 5% of your lost weight
- You can identify specific behavior changes (stopped tracking protein, skipped workouts, sleep got worse)
- Your appetite increase is moderate and manageable
- You haven't been consistent with the lifestyle anchors above
Consider Restarting If:
- You've regained more than 10% of your lost weight despite consistent lifestyle efforts
- Your appetite is uncontrollable and impacting quality of life
- You're experiencing metabolic changes (fasting glucose climbing, lipids worsening)
- You've given lifestyle-only maintenance a genuine 3-6 month effort
Restarting doesn't mean failure. If anything, the data suggests that for many people, some level of pharmacological support is appropriate long-term. The stigma around "needing medication to maintain weight loss" makes about as much sense as stigmatizing someone for staying on thyroid medication.
The Psychological Side of Stopping
Nobody talks about this enough.
Stopping a GLP-1 can feel like losing a superpower. For months, maybe for the first time in your life, food didn't control you. You could walk past the kitchen without thinking about what's in the fridge. You could eat a normal portion and feel satisfied. You could focus on your day without the constant background hum of "when's the next meal?"
When that goes away, it hits hard. And it's not just the physical hunger returning. It's the emotional weight of realizing that your relationship with food might always require active management.
This is normal. It doesn't mean you're weak or that the medication was a crutch. It means you have a physiology that requires either pharmacological support or very deliberate lifestyle strategies (or both) to maintain a healthy weight.
Reframe the narrative
You didn't "fail" if you need ongoing support. You learned what your body needs. That's information, not a verdict.
Find your non-food rewards
While on a GLP-1, many people lose interest in food as a source of pleasure. You need to replace that with something: exercise, hobbies, social connection.
Track your wins, not just your weight
Strength gains in the gym, energy levels, lab improvements, clothing fit. Weight is one data point. It shouldn't be the only measure of whether this is working.
Frequently Asked Questions
Disclaimer: This article is for educational purposes only and is not medical advice. Always consult a qualified healthcare provider before making changes to your GLP-1 protocol. Individual responses to weight loss medications vary. Proper medical supervision is recommended for any tapering or discontinuation plan.
Ready to track your protocol?
- Smart reminders so you never miss a dose
- Track weight, photos, and progress over time
- Medication level curves for every compound