GLP-1 Muscle Loss: How to Protect Lean Mass on Ozempic, Mounjaro, or Zepbound
The Bottom Line
GLP-1 medications like semaglutide and tirzepatide cause significant weight loss, but not all of that weight is fat. Clinical trials show that 25-40% of total weight lost can be lean mass (muscle, bone density, organ tissue). That matters because losing muscle tanks your metabolism, makes weight regain more likely, and affects how you look and feel long-term. The fix isn't complicated: high protein intake, consistent resistance training, and tracking body composition instead of just scale weight. Track your body composition, protein intake, and training alongside your GLP-1 protocol with the Regimen app.
In this guide:
The Muscle Loss Reality: What the Clinical Data Shows
Every diet causes some muscle loss. That's a basic biological reality of caloric deficit. But GLP-1s create unusually aggressive deficits because they suppress appetite so effectively that many people are eating far less than they realize.
SURMOUNT-1 (tirzepatide)
Participants lost an average of 20.9% total body weight. Of that, approximately 26% was lean body mass. For someone who lost 50 lbs, that means roughly 13 lbs of muscle and other lean tissue.
STEP 1 (semaglutide 2.4mg)
Average weight loss of 14.9% body weight. Body composition substudies showed lean mass accounted for about 25-39% of total weight lost, depending on the measurement method.
For comparison, well-designed caloric restriction with adequate protein and resistance training typically results in only 10-15% of weight lost coming from lean mass. The difference is substantial.
Why GLP-1s Cause Muscle Loss
Three mechanisms work together to create the muscle loss problem.
Severe Caloric Deficit
The average person on a therapeutic dose reduces their calorie intake by 25-40%. Many don't realize how little they're eating because the appetite suppression feels natural. But your muscles don't care that you're not hungry. They need amino acids to maintain themselves.
Reduced Protein Absorption
GLP-1s slow gastric emptying, which means food moves through your system more slowly. Many people on GLP-1s report that protein-heavy meals feel uncomfortable, heavy, and hard to finish. The result is that they gravitate toward lighter, easier-to-eat foods that tend to be lower in protein.
Anabolic Signaling Reduction
Being in a sustained caloric deficit downregulates mTOR, the primary signaling pathway for muscle protein synthesis. Your body shifts into conservation mode: break down tissue you're not actively using, preserve energy stores. Without the stimulus of resistance training to tell your body "keep this muscle, I need it," your body will preferentially sacrifice lean mass.
The Protein Solution
Protein intake is the most controllable factor in whether you lose mostly fat or a mix of fat and muscle on GLP-1s.
How Much Protein You Need
- Minimum: 1.2g per kg of body weight per day
- Better: 1.4-1.6g per kg of body weight per day
- For serious lifters: Up to 2.0g per kg
For a 200 lb (91 kg) person, that's 109-145g of protein daily at the recommended range.
The Leucine Threshold
Not all protein servings are equal. Each meal needs to hit a leucine threshold of about 2.5-3g to maximally stimulate muscle protein synthesis. In practical terms, each protein-containing meal should have at least 25-35g of complete protein. Three meals at 30-40g of protein each will do more for your muscles than the same total spread across six small snacks.
Practical Protein Strategies for GLP-1 Users
Protein first, always. Start every meal with the protein. If you can only eat half your plate before feeling full, make sure the protein was the half you ate.
Liquid protein is your friend. When solid food feels heavy, a protein shake delivers 25-40g in a form that's easier on a sluggish stomach.
Front-load your day. Aim for 30-40g at your first meal. Many GLP-1 users find their appetite is strongest in the morning.
Greek yogurt, cottage cheese, and eggs are high-protein foods that most GLP-1 users tolerate well because they're relatively easy to digest.
Resistance Training: Your Non-Negotiable Defense
Protein provides the raw materials. Resistance training provides the signal that tells your body to keep the muscle. Without that signal, your body looks at the caloric deficit and makes a rational decision: break down tissue you aren't using.
The Minimum Effective Dose
- Frequency: 2-3 sessions per week, minimum. Each major muscle group trained at least twice per week.
- Exercise selection: Prioritize compound movements: squats/leg press, deadlifts, bench press/push-ups, rows, overhead press, pull-ups/lat pulldowns.
- Intensity: Lift heavy enough that the last 2-3 reps of each set are genuinely challenging.
- Volume: 2-4 sets per exercise, 6-12 reps per set. Total of 10-20 sets per muscle group per week.
Training on Low Appetite
Training when you're eating less feels different. You'll have less energy, your recovery might be slower, and your strength may plateau or even dip. That's fine. The goal during GLP-1 treatment isn't to set PRs. The goal is to maintain your current strength levels, which tells your body to preserve the muscle you have.
Body Composition Tracking: Why the Scale Lies
If you lose 10 lbs of fat and 5 lbs of muscle, the scale says you lost 15 lbs. If you lose 13 lbs of fat and 2 lbs of muscle, the scale also says you lost 15 lbs. Same number, completely different outcome.
A DEXA scan is the gold standard ($75-150 per scan). Get one before starting your GLP-1 and repeat every 3-4 months. InBody or bioelectrical impedance scales are less accurate but useful for tracking trends.
Measure your waist at the navel and hips at the widest point. This ratio tracks fat distribution changes that matter for metabolic health.
Track your working weights on 3-4 key lifts. If they're maintaining while you lose weight, you're preserving muscle. If they're dropping consistently, increase protein or training stimulus.
Take them monthly in consistent lighting and poses. The mirror lies less than the scale.
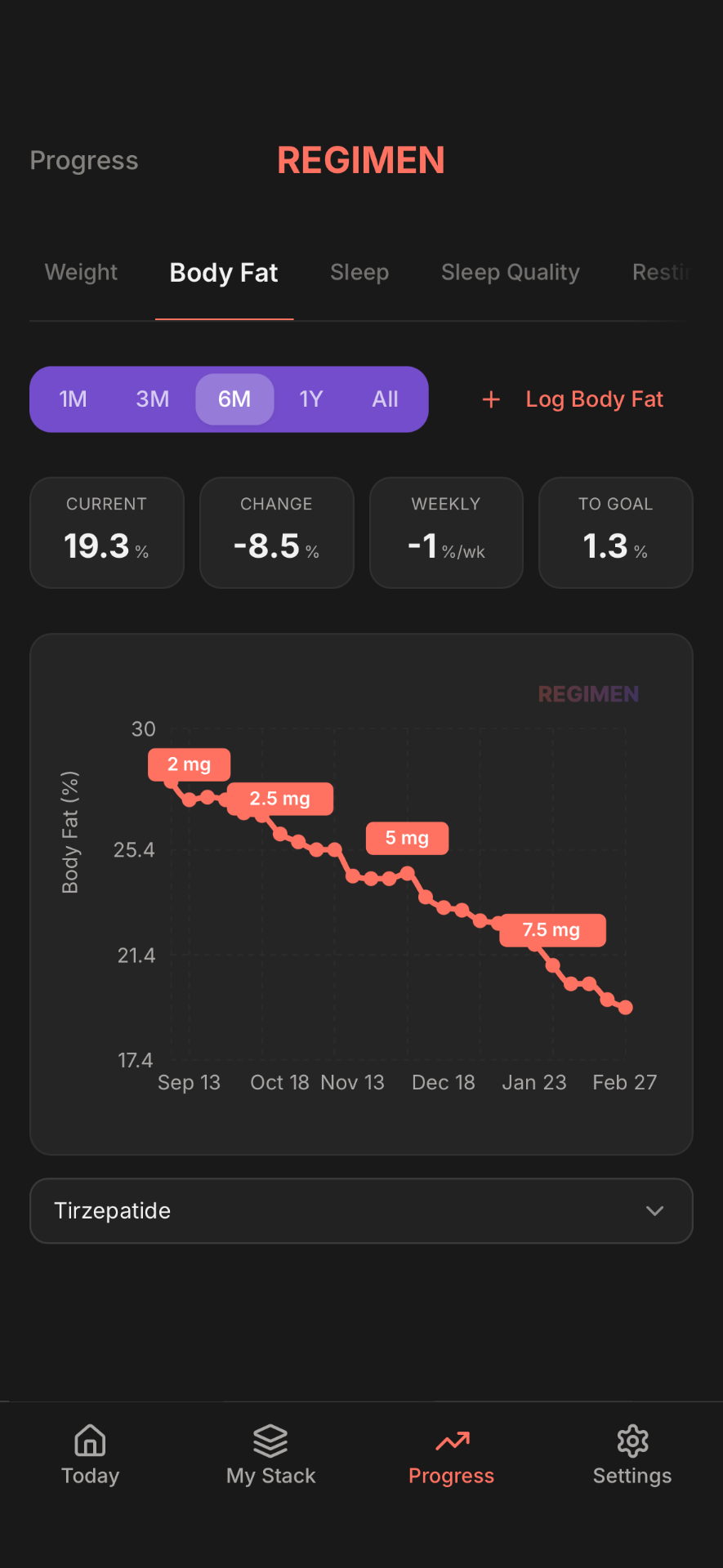
Track body composition alongside your GLP-1 protocol
- Log weight, body fat, and strength benchmarks
- See body composition trends over time
- Catch muscle loss early and adjust your strategy
Supplements That Actually Help
Most supplements marketed for muscle preservation are garbage. Here's what actually has evidence behind it.
Creatine Monohydrate
The most researched supplement in sports science. Supports muscle energy during resistance training, has a meaningful effect on lean mass preservation during caloric deficit, and improves recovery. Dose: 3-5g daily. No loading phase needed. It will add 2-4 lbs of water weight in the first 1-2 weeks (intracellular water, not bloating).
Protein Supplements
Whey protein isolate is the most effective for muscle protein synthesis. Casein before bed provides slower overnight release. Use supplements to hit your target when whole food falls short.
HMB (Beta-Hydroxy Beta-Methylbutyrate)
A metabolite of leucine with some evidence for reducing muscle protein breakdown during caloric restriction. Dose: 3g daily, split into 1g with meals. Not a substitute for adequate protein and training, but may provide additional benefit.
What Doesn't Help
- BCAAs: Redundant if you're eating adequate protein. Save your money.
- Testosterone boosters: OTC test boosters don't meaningfully impact muscle preservation. If you have clinically low testosterone, talk to your doctor.
- Fat burners: You're already in a significant caloric deficit from the GLP-1. Adding stimulants increases muscle breakdown risk.
Tirzepatide vs Semaglutide for Muscle Preservation
There's growing interest in whether tirzepatide or semaglutide is better for body composition. The data so far suggests a slight advantage for tirzepatide, but it's not as clear-cut as some influencers claim.
| Factor | Semaglutide | Tirzepatide |
|---|---|---|
| Total weight loss | 14-17% body weight | 20-26% body weight |
| Lean mass as % of total loss | 25-39% | ~26% |
| Fat mass loss | Higher % of loss is fat | Similar % |
| GIP receptor activity | None | Yes (dual agonist) |
Tirzepatide's GIP receptor activity may provide some degree of muscle preservation. But the research is early and the differences are modest. Don't choose between tirzepatide and semaglutide based solely on muscle preservation. Both require the same protective strategies. The compound you use matters less than the lifestyle you pair it with.
Frequently Asked Questions
Disclaimer: This article is for educational purposes only and is not medical advice. Always consult a qualified healthcare provider before making changes to your diet, exercise, or medication protocol. Individual responses to GLP-1 medications vary. Proper medical supervision is recommended.
Ready to track your protocol?
- Smart reminders so you never miss a dose
- Track weight, photos, and progress over time
- Medication level curves for every compound