TRT Bloodwork Guide: What Labs to Get, When to Test, and How to Read Your Results
Your doctor checks your total testosterone once a quarter, glances at the number, and says "looks good." But some weeks you feel dialed in, full of energy and motivation, and other weeks you're dragging, bloated, or irritable for no obvious reason.
That disconnect isn't random. It's almost always traceable to something in your protocol: injection timing, estrogen fluctuations, hematocrit creeping up, or a dose change you made three weeks ago that's finally catching up.
The problem? Most guys on TRT don't track any of this. They inject, forget, and then sit in front of their doctor unable to answer basic questions about how they've been feeling, when they last changed their dose, or what their symptoms looked like before the adjustment.
This guide covers everything you should be monitoring on TRT, from bloodwork panels to daily subjective metrics, and how to connect the dots between your protocol and how you actually feel.
The Full TRT Bloodwork Panel
Most TRT clinics check total testosterone and maybe a CBC. That's not enough. Here's the full panel you should be getting and why each marker matters when you're on exogenous testosterone.
| Marker | Why It Matters on TRT | Target Range | Red Flags |
|---|---|---|---|
| Total Testosterone | Your overall testosterone level | 600-1100 ng/dL (at trough) | Below 400 or above 1500 at trough |
| Free Testosterone | The testosterone actually available for use. Total T can look good while free T is low due to high SHBG | 15-25 pg/mL | Below 10 despite adequate total T |
| Estradiol (E2) | Testosterone converts to estrogen via aromatase. Too high or too low causes problems | 20-40 pg/mL (sensitive assay) | Below 15 or above 50 with symptoms |
| SHBG | Sex hormone-binding globulin. Binds testosterone and makes it unavailable. Affects how much free T you have | 20-50 nmol/L | Below 15 (often from insulin resistance) or above 60 |
| Hematocrit (HCT) | TRT increases red blood cell production. High HCT thickens blood and increases cardiovascular risk | Below 52% | Above 54% (donate blood, lower dose, or increase injection frequency) |
| CBC (Complete Blood Count) | Monitors red and white blood cells, hemoglobin, and platelets alongside hematocrit | Within lab reference ranges | Polycythemia (elevated RBCs across the board) |
| PSA | Prostate-specific antigen. TRT doesn't cause prostate cancer, but it can accelerate existing issues | Below 4.0 ng/mL | Rapid increase (more than 1.0 in 12 months) |
| Lipid Panel | TRT can negatively affect HDL cholesterol in some men | HDL above 40, LDL below 130 | HDL dropping below 30 or significant LDL increase |
| Liver Enzymes (AST/ALT) | Baseline monitoring. Oral testosterone (rare) and some ancillaries can stress the liver | Within lab reference ranges | Persistently elevated above 2x normal |
Pro tip: Always request the sensitive estradiol assay (LC/MS-MS), not the standard immunoassay. The standard assay is designed for women and can be wildly inaccurate for men, especially at the lower end. Quest Diagnostics test code 30289 is the one you want.
When to Get Labs (and Why Timing Matters)
The same protocol can produce wildly different lab numbers depending on when you get blood drawn. Understanding this prevents unnecessary dose changes based on misleading data.
Trough vs. Peak Testing
If you inject testosterone cypionate on Monday morning and get labs Monday afternoon, your levels are at their peak. If you get labs Friday morning (right before your next injection), you're at your trough. The difference can be 400+ ng/dL.
Standard practice: Get bloodwork at your trough, the morning before your next scheduled injection. This gives you your lowest point, which is what most clinical ranges are based on and what your doctor needs to make dosing decisions.
The Timing Rules
- Time of day: Morning, ideally 7-10 AM. Testosterone has a natural diurnal rhythm (even on TRT), and morning draws give the most consistent results
- Fasting: Fast for 8-12 hours before labs. This ensures accurate lipid and glucose readings
- After dose changes: Wait at least 6-8 weeks after any protocol change before retesting. Testosterone cypionate has an apparent serum half-life of about 6.9 days, so it takes 5-6 half-lives (roughly 5-6 weeks) to reach new steady state
- PSA note: Avoid ejaculation 24-48 hours before PSA testing, and don't get labs the day after heavy lower-body training. Both can falsely elevate PSA
Lab Schedule
| When | What to Test |
|---|---|
| Before starting TRT | Full panel (everything in the table above) plus LH, FSH as baseline |
| 6-8 weeks after starting | Full panel. This is your first checkpoint |
| 6-8 weeks after any dose change | Total T, Free T, E2, HCT at minimum |
| Every 3-6 months (once stable) | Total T, Free T, E2, HCT, CBC, lipids |
| Annually | Full comprehensive panel including PSA, liver enzymes, metabolic panel |
Beyond Bloodwork: Daily Metrics That Actually Matter
Labs tell you what's happening in your blood. But they only capture a single moment every few months. The space between labs is where the real optimization happens, and that requires tracking how you feel day to day.
Here's what's worth monitoring and why:
- Energy levels: Consistent low energy mid-week on a once-weekly injection could mean your levels are dropping too far. That pattern only becomes visible if you log it
- Sleep quality: Both high and low estrogen disrupt sleep. If you notice poor sleep 2-3 days after injection (when E2 peaks), that's a data point
- Libido: Often the first thing to change when something's off. A sudden drop after adding or adjusting an aromatase inhibitor is a classic sign of crashed estrogen
- Mood and irritability: TRT should stabilize mood. If you're experiencing mood swings, it usually points to unstable hormone levels (often from infrequent injections or E2 fluctuations)
- Morning erections: Yes, this is a legitimate clinical marker. Consistent morning erections indicate healthy testosterone and estrogen balance. Their absence often precedes lab changes
- Water retention / bloating: Often the first visible sign of elevated estrogen. Track this alongside your injection schedule
- Acne and skin oiliness: Can indicate high DHT conversion or fluctuating hormone levels. More common with infrequent injection schedules
- Injection site reactions: Tracking which sites you use and any reactions helps you build a rotation pattern. You can log injection sites in your notes to maintain a consistent rotation between areas like glutes, ventrogluteal, deltoids, and quads
The real power is correlation. When you can look back and see "I felt great the two weeks after increasing my dose by 20mg, then mood dropped as E2 climbed," you have actionable data for your next doctor visit.
The Multi-Compound Reality
If you're only on testosterone, feel free to skip ahead. But the reality is that most TRT patients end up managing multiple compounds:
HCG (Human Chorionic Gonadotropin)
HCG mimics luteinizing hormone (LH) and keeps your testes producing a small amount of testosterone and other hormones locally. It's commonly prescribed alongside TRT for:
- Fertility preservation: TRT suppresses sperm production. HCG maintains some intratesticular testosterone, which is needed for spermatogenesis
- Testicular size: Without HCG, testicles gradually atrophy on TRT. Most men don't want that
- Neurosteroid support: The testes produce pregnenolone and DHEA, which have downstream effects on mood and cognition. HCG helps maintain this pathway
Typical dosing: 250-500 IU, 2-3 times per week. That's another 2-3 injections on top of your testosterone schedule. Tracking which days you take what, and at what dose, becomes important fast.
Aromatase Inhibitors (AIs)
Anastrozole (Arimidex) is the most commonly prescribed AI on TRT. It blocks the enzyme that converts testosterone to estrogen. The key point: most men on properly dosed TRT don't need an AI.
But some do, particularly men with higher body fat (more aromatase enzyme), higher doses, or those who are genetically strong aromatizers. If you do use an AI, tracking symptoms is essential because the line between "just right" and "crashed estrogen" is thin.
Other Common Ancillaries
- DHEA (25-50mg daily): Often added to replace what the testes would normally produce. Some clinics include it routinely
- Pregnenolone (50-100mg daily): Upstream hormone that supports cognitive function and other steroid pathways
- Finasteride/Dutasteride: 5-alpha reductase inhibitors for men experiencing hair loss on TRT. These reduce DHT conversion
When you're managing testosterone, HCG, and possibly an AI, that's three different compounds with different injection schedules and doses. This is where tracking becomes non-negotiable.
Estrogen: The Most Misunderstood Part of TRT
Estrogen management causes more confusion in the TRT community than almost anything else. Here's what you need to know.
Why Estrogen Matters
Men need estrogen. It's essential for bone density, cardiovascular health, joint health, cognitive function, and libido. The goal on TRT is not to eliminate estrogen. It's to keep it in a range where you feel good and don't experience side effects.
Signs of High Estrogen
- Water retention and bloating (especially face and midsection)
- Mood swings, emotional sensitivity
- Nipple sensitivity or gynecomastia
- Decreased libido (paradoxically)
- Increased blood pressure from water retention
- Poor sleep quality
Signs of Low Estrogen (Often From Over-Using an AI)
- Joint pain and cracking (this is the hallmark sign)
- Extreme fatigue and lethargy
- Depression, flat mood, no motivation
- Dry skin and lips
- Complete loss of libido
- Erectile dysfunction
- Bone density concerns long-term
Important: Low estrogen from an AI often feels worse than mildly high estrogen. Many experienced TRT users and clinicians now recommend not using an AI unless symptoms are significant and confirmed with bloodwork. If your E2 is 45 but you feel great, there's likely no reason to take an AI.
Managing Estrogen Without an AI
Before reaching for anastrozole, try these approaches first:
- Increase injection frequency: Splitting your weekly dose into 2-3 injections creates smaller peaks and less aromatization
- Lower body fat: Adipose tissue contains aromatase. Losing body fat naturally reduces conversion
- Adjust dose: Sometimes a slightly lower testosterone dose with better estrogen balance produces better results than a higher dose with AI dependency
- DIM and calcium d-glucarate: Mild natural estrogen metabolizers that some men find helpful for borderline cases
Injection Frequency and Stable Levels
The debate around injection frequency is one of the most common topics in TRT forums, and for good reason. How often you inject directly affects hormone stability, side effects, and how you feel.
The Science of Frequency
Testosterone cypionate has an apparent serum half-life of about 6.9 days (older references quote ~8 days; reconciled here). With a once-weekly injection, you get a noticeable peak 24-48 hours after injection, followed by a steady decline. By day 7, levels have dropped noticeably. Many men feel great for days 1-4 and then experience fatigue, mood dips, or irritability as levels fall.
| Frequency | Pros | Cons |
|---|---|---|
| Once weekly | Fewer injections, simpler schedule | Larger peaks and troughs, more E2 spikes, more side effects |
| Twice weekly | More stable levels, less aromatization, fewer mood swings | More injections per week |
| Every other day (EOD) | Very stable levels, minimal E2 issues, often eliminates AI need | More frequent injections, requires good tracking |
| Daily (micro-dosing) | Most stable levels possible, mimics natural production | Daily commitment, usually requires insulin syringes with smaller needles |
The general trend in TRT optimization: more frequent, smaller injections tend to reduce side effects. This is because smaller doses create less of an E2 spike, keep hematocrit more stable, and provide a more consistent hormonal environment. For a deep dive into how to implement this, see our guide on microdosing TRT protocols.
If you're on the fence about switching to more frequent injections, just try it for 6 weeks. Most guys who switch never go back.
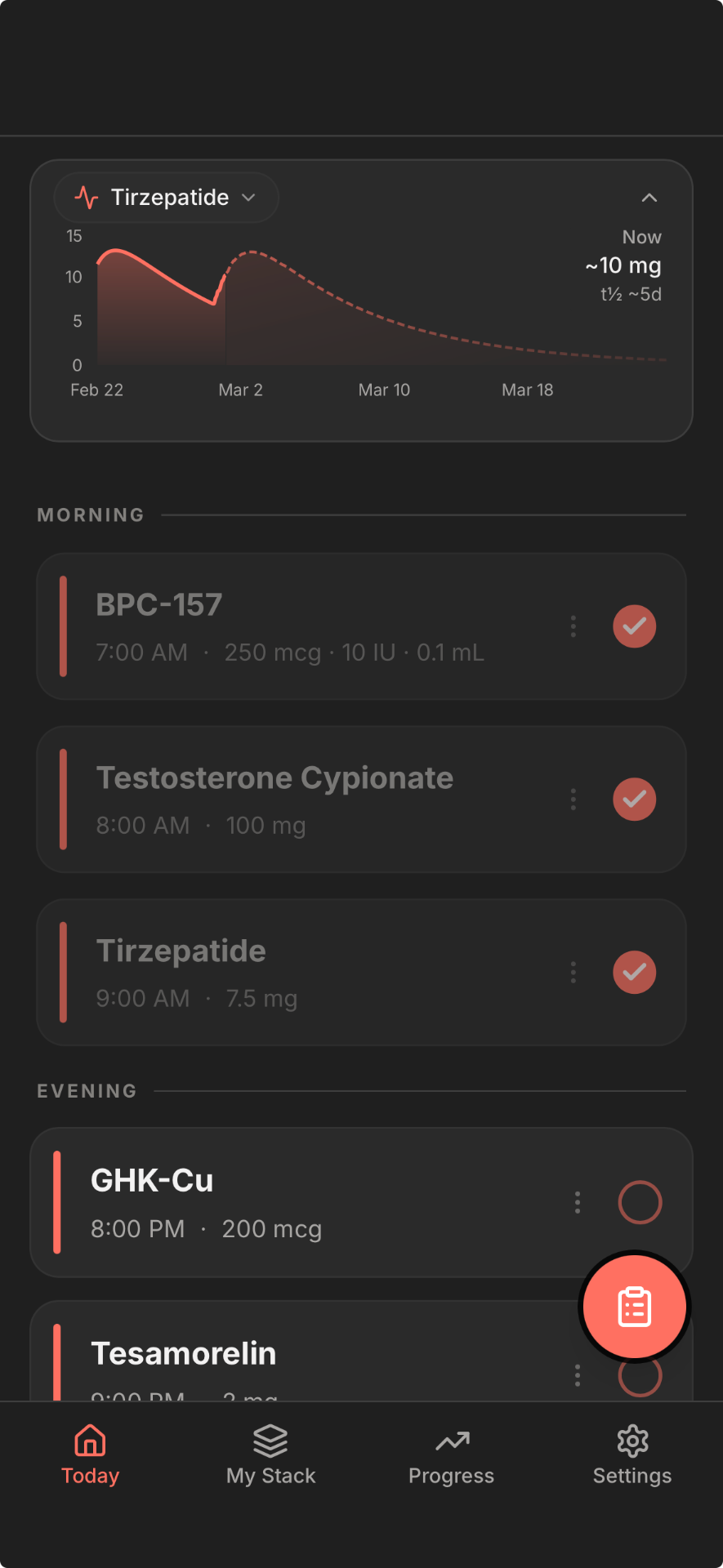
A medication level visualization can make this concept tangible. When you see the curve of your testosterone levels between injections, it becomes obvious why you feel different on day 2 versus day 6 of a weekly protocol. An app like Regimen shows these half-life curves so you can see exactly when your levels peak and drop.
How to Actually Track All of This
Having the knowledge above is step one. But information without implementation is useless. Here's how to put a practical tracking system in place.
What Your Tracking System Needs
- Multi-compound support: If you're on testosterone + HCG + an AI, you need to track three different medications with different schedules. Generic health apps don't handle this well
- Dose flexibility: You should be able to set up your protocol by weekly total and frequency (e.g., 150mg/week split into 2 injections) or log individual injections. Both approaches are valid depending on how you think about your protocol
- Oil-based calculator: For testosterone cypionate and enanthate, an oil-based calculator helps you convert between different concentrations (200mg/mL vs 250mg/mL) and calculate exact injection volumes
- Medication level visualization: Being able to see your testosterone levels plotted over time based on half-life data helps you understand the peaks and troughs in your protocol
- Symptom correlation: The ability to track energy, mood, sleep, and libido alongside your injection log so you can spot patterns between dose changes and how you feel
- Reminders: Especially important for multi-compound protocols where you're injecting on different days
- Dose change history: When you change from 150mg to 180mg per week, you want a clear record of when that happened so you can correlate it with lab results and symptom changes
Regimen was built specifically for protocols like this. It handles multi-compound tracking, medication level curves, the TRT dose calculator for reconstitution and dosing math, and progress correlation between your protocol and daily metrics.
Common TRT Mistakes
After years of community feedback and clinical guidance, these are the mistakes that come up repeatedly:
- Chasing numbers instead of symptoms. If you feel great at 700 ng/dL, don't chase 1200 because someone on the internet said higher is better. The goal is optimal symptoms, not a specific number. Some men feel best at 600, others at 1000.
- Getting labs at the wrong time. Testing at peak gives you inflated numbers that lead to unnecessary dose reductions. Testing randomly (afternoon, non-fasting) gives inconsistent data. Standardize your lab timing.
- Changing doses too frequently. The 6-8 week rule exists because it takes that long to reach steady state. Changing your dose every 2-3 weeks based on how you feel means you never actually know what any given dose does for you.
- Ignoring hematocrit. High hematocrit is the most common tangible health risk on TRT. It increases blood viscosity and cardiovascular risk. Monitor it, and if it climbs, address it proactively with hydration, grapefruit naringin, blood donation, or dose/frequency adjustments.
- Pre-emptive AI use. Taking an aromatase inhibitor "just in case" without symptoms or elevated E2 on bloodwork can crash your estrogen and make you feel significantly worse than mildly elevated E2 would.
- Not tracking anything. Relying on memory for injection dates, doses, and how you felt is unreliable. Six months from now, you won't remember whether you felt better on 140mg or 160mg per week. Data does remember.
- Comparing your labs to everyone else's. Individual response to TRT varies enormously based on SHBG, body composition, genetics, and aromatase activity. Your optimal protocol is yours, informed by your data.
Frequently Asked Questions
What bloodwork should I get on TRT?
At minimum: Total Testosterone, Free Testosterone, Estradiol (sensitive assay), SHBG, Hematocrit, CBC, PSA, and a lipid panel. Comprehensive annual panels should also include liver enzymes (AST/ALT) and a metabolic panel. Always test at trough (before your next injection) in the morning.
How often should I get labs on TRT?
6-8 weeks after starting or after any dose change. Once stable, every 3-6 months for core markers (Total T, Free T, E2, HCT) and annually for a comprehensive panel. More frequent testing is warranted if you're experiencing symptoms or making protocol adjustments.
Should I get bloodwork at trough or peak on TRT?
Trough (the morning before your next scheduled injection). This gives you your lowest levels, which is the standard clinical reference point. Testing at peak can show levels 400+ ng/dL higher and lead to unnecessary dose reductions. Consistency in timing is more important than which point you choose, but trough is the standard.
How do I know if my estrogen is too high on TRT?
Look for symptoms: water retention, bloating, nipple sensitivity, mood swings, decreased libido, or poor sleep. Then confirm with bloodwork using the sensitive estradiol assay (LC/MS-MS). The number alone doesn't tell the full story. Some men feel fine at E2 of 50 pg/mL while others have symptoms at 35. Track symptoms alongside labs to find your personal sweet spot.
Can I track TRT and HCG together in one app?
Yes. Regimen supports multi-compound tracking, so you can log testosterone, HCG, an aromatase inhibitor, and any other medications or supplements in your protocol. Each compound gets its own schedule, dose tracking, and medication level curve.
How long should I wait to adjust my TRT dose?
A minimum of 6-8 weeks. Testosterone cypionate has an apparent serum half-life of about 6.9 days, so it takes approximately 5-6 half-lives (roughly 5-6 weeks) to reach a new steady state after a dose change. Adjusting sooner means you're reacting to incomplete data. The exception is if you're experiencing significant side effects that require immediate intervention, in which case work with your prescribing physician.
Related Tools
Start with our free TRT dose calculator
Calculate your injection volume based on concentration and dose
Track your injections with the Regimen app
Log doses, set reminders, and correlate with labs
TRT Dose Calculator
Calculate injection doses for cypionate, enanthate, and propionate
TRT Tracker
Track your full TRT protocol with medication levels
Ready to track your protocol?
- Smart reminders so you never miss a dose
- Track weight, photos, and progress over time
- Medication level curves for every compound